

CPR, First Aid, BLS, ACLS, PALS certifications.


The symptoms associated with ACS include:
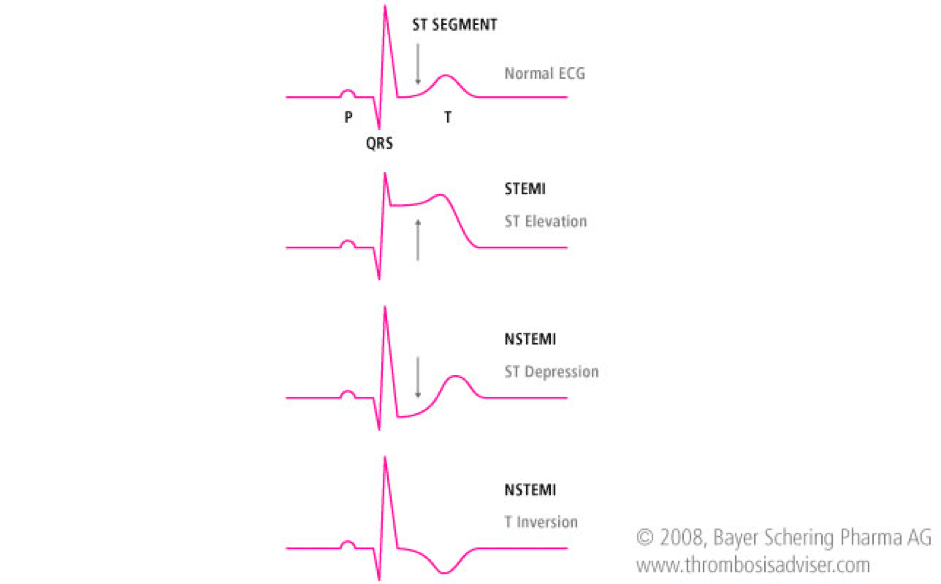
ST-Segment Elevation Myocardial Infarction (STEMI) is an elevation > 1mm in 2 or more contiguous or greater than 2 mm in leads V2 and V3.
Unstable Angina (UA) or Non ST-Elevation Myocardial Infarction (NSTEMI) is a depression ≥0.5 mm or greater T-wave inversion.
Low Risk Unstable Angina (UA) is an ST segment deviation of <0.5 mm or T wave inversion of 2 mm. Patients may also have normal ECGs.
Scenario: A 70-year patient comes to the hospital and is complaining of chest pain radiating to his arm and he seems very anxious and out of breath.
Assessment:
Interventions:
Management:
Treatments which are used in ACLS algorithm for ACS are:

